Reproductive Justice Media Reference Guide
a guide for reporting on abortion and the Latinx community
Introduction
This Reproductive Justice Media Guide is intended to be used by members of the media seeking to learn about or expand their knowledge of reproductive justice particularly when reporting on abortion and the Latinx community. It is not intended to be an all-inclusive encyclopedia of issues within reproductive justice, nor is it intended to limit coverage to the issues highlighted herein. We hope this is a conversation starter and will yield more nuanced discussions and reporting about abortion and reproductive justice more broadly.
Members of the media have tremendous power in shaping the public’s understanding of reproductive justice issues. In covering stories about reproductive health and rights, journalists can ask three questions to explore the possible reproductive justice implications.
- Are women of color, young people, immigrants, LGBTQ individuals, or low-income communities being disproportionately affected in a way that warrants exploration? Are certain communities or populations experiencing a significant difference in outcomes than others?
- Who are the experts from communities affected by systemic disparities who can serve as sources or provide a first-hand perspective for the story? Experts can be academics or professionals but should also include people from affected communities with lived experience in this issue.
- What are the historic factors that contribute to systemic disparities and disproportionate outcomes? In many instances, including law, policy, and intervention by the medical establishment, legacies of racism and colonialism have created disparities that provide critical context in understanding today’s outcomes.
Reproductive health and rights face consistent attacks in the United States regardless of the political party in power; however, at both the state and federal level, high-profile conservative politicians are intent on dismantling basic health care rights. These efforts combined with a strong anti-immigrant sentiment mean it is critical to develop a strong understanding of how reproductive healthcare particularly impacts Latinx and immigrant communities. (See the sidebar, “On Gender and Latino/Latina/Latinx.”)
Media coverage of reproductive rights and health issues often centers on the controversy around the legal right to abortion. This narrow focus leaves out many of the experiences and priorities of women of color, young people, immigrant communities, LGBTQ families, and others who are affected by the broad range of issues of reproductive justice.
On Gender and Latino/Latina/Latinx
Throughout this guide, we incorporate gender-neutral language to discuss abortion and reproductive issues. In other words, we say “a pregnant person,” rather than “a pregnant woman.” We do this because transgender men and gender non-conforming (GNC) people can also be pregnant. At the same time, we are aware that using gender-neutral language does not always highlight the disproportionate impact of abortion policies on women, institutionalized sexism, and the many efforts to undermine the self-determination and autonomy of all women, including transgender women. In addition, most statistics cited use the term woman because of current limits of data collection as it relates to gender identity. Therefore, all statistics cited use the terminology from the original poll, survey, health data set, or original source.
The term Latinx has gained traction among activists, academics, and millennials, while many other Latinas/os don’t necessarily identify with this terminology. Latinx refers to a person of Latin-American origin or descent. The “x” makes the masculine identifier Latino and the feminine Latina gender-neutral and non-binary. Latinx goes beyond Latin@, which has been used to include both masculine and feminine identities, challenging the gender binary in the Spanish language. Dropping the a/o structure, Latinx embraces the diversity of genders that often are actively erased from many reproductive health and rights conversations. Pronounced “La-teen-ex,” this term includes the numerous people of Latin-American descent whose gender identities fluctuate along different points of the spectrum, from agender or non-binary to gender non-conforming, genderqueer, and genderfluid.1 To be inclusive of all gender identities, we use Latinx to refer to someone from the Latino community throughout this guide. When citing data about the Latinx community, we use the term originally used by the pollster or cited in the data. Therefore, we also use the terms Hispanic(s), Latina(s), Latino(s), and Latin@(s) in this document.
Defining Reproductive Justice
Forward Together and our partners who co-authored this guide (California Coalition for Reproductive Freedom, California Latinas for Reproductive Justice, Colorado Organization for Latina Opportunity and Reproductive Rights, and the National Latina Institute for Reproductive Health) define reproductive justice as:
re • pro • duc • tive just • tice
All people having the social, political, and economic power and resources to make healthy decisions about their gender, bodies, sexuality, and families for themselves and their communities.
From abortion access to the rights of incarcerated individuals and resources for young families, reproductive justice issues run the gamut. Though reproductive justice is expansive, it is more than a container for a set of issues; it is an analytic framework and a social movement for self-determination.
The reproductive justice framework was created in 1994 by Black women social justice leaders after attending the International Conference for Population and Development in Cairo, Egypt. They saw international women activists using a human rights framework (including economic justice, the right to education and healthcare, and to be free from violence) to push for the same rights that they were fighting for in the United States. These movement leaders spliced together “reproductive rights” and “social justice” to create “reproductive justice,” a human rights way of “looking at the totality of women’s lives.”2 Reproductive justice activists treat abortion and other reproductive health services as akin to the resources all human beings are entitled to—such as healthcare, education, housing, and food—in an equitable, democratic society.3 Reproductive justice provides an approach to understanding that reproductive health and decisions must be contextualized, and that centering underrepresented voices is critical to defining the problem, posing solutions, and leading the movement for change. (See the sidebar, “What’s the difference between reproductive health, reproductive rights, and reproductive justice?”)
What’s the difference between reproductive health, reproductive rights, and reproductive justice?
The reproductive health framework centers around healthcare service delivery. The focus is on providing services for historically marginalized communities through the creation of reproductive health clinics that provide low- or no-cost care, as well as culturally competent services. Underserved communities face a lack of access, not only to reproductive health services, but also to all healthcare. For many women, reproductive healthcare is their first and perhaps only encounter with the healthcare system.4
The reproductive rights framework is a legal and advocacy-based model that serves to protect an individual woman’s legal right to reproductive healthcare services with a focus on keeping abortion legal and increasing access to family planning services. Groups fight for a woman’s “right to choose” and “right to privacy” through various legal, advocacy, and political means.5
The reproductive justice framework is rooted in the recognition of the histories of reproductive oppression and abuse in communities of color. This framework uses a model grounded in organizing women, girls, and gender non-conforming (GNC) people to change structural power inequalities. The central theme of the reproductive justice framework is a focus on naming and eliminating the control and exploitation of women’s bodies, sexuality, and reproduction as an effective strategy of controlling people, particularly women of color, trans and GNC people of color, and their communities.6 In response to transphobia and specifically transmisogyny within the reproductive health and rights movements, reproductive justice advocates have been making an effort to expand the framework to include trans and GNC people.
“Reproductive justice is a positive approach that links sexuality, health, and human rights to social justice movements by placing abortion and reproductive health issues in the larger context of the well-being and health of women, families and communities. It posits that the ability of any woman to determine her own reproductive destiny is directly linked to the conditions in her community and these conditions are not just a matter of individual choice and access. This is in contrast to traditional reproductive rights messaging. Reproductive justice addresses issues of population control, bodily self-determination, immigrants’ rights, economic and environmental justice, sovereignty, and militarism and criminal injustices that limit individual human rights because of group or community oppressions.”7
In Focus: Abortion

United States Induced Abortion Facts8
- Of all pregnancies among U.S. women in 2011, 45%—nearly half—were unintended. About 4 in 10 of these pregnancies were terminated by abortion.
- Hispanics accounted for 25% of abortion procedures in 2014.
- The abortion rate in 2014 was 14.6 abortions per 1,000 women aged 15–44, down 14% from 16.9 per 1,000 in 2011. So the parallel statement would be: Between 2011 and 2014, abortion rates fell by 14%.
- A first-trimester abortion carries minimal risk—less than 0.05%—of major complications leading to hospital care, making it one of the safest medical procedures.
- Of abortions obtained in 2014, 59% were by patients who had also had at least one birth.
- In 2014, some 75% of abortion patients were poor or low-income; 26% had incomes of 100–199% of the federal poverty level; and 49% had incomes of less than 100% of the federal poverty level ($15,730 for a two-person family).
- In 2014, 90% of all U.S. counties had no clinic, and 39% of women of reproductive age lived in those counties.
- In 2011, 84% of clinics reported anti-abortion harassment: 80% reported being picketed, with 53% reporting being picketed 20 times or more in a year, 47% reported receiving harassing phone calls, and 3% reporting receiving at least one bomb threat.
Latin America and the Caribbean: Abortion Access Facts
Understanding Latinx perspectives and experiences on abortion in the U.S. requires some understanding of the context of abortion in Latin America and the Caribbean. The Guttmacher Institute reports that “More than 97% of women of childbearing age in Latin America and the Caribbean live in countries where abortion is restricted or banned altogether.”9 When reporting on various Latinx communities, it is important to consider the legality and attitudes about abortion in their countries of origin, and to remain open to how law and culture may affect personal beliefs, particularly for recent immigrants.For many recent Latinx immigrants, legal abortion access in the United States is completely new. Additionally, opinions and experiences around reproductive health and abortion access must be considered in the context of reproductive health services usage, which includes abortion.
- Incidence of inducing nonsurgical abortions with misoprostol is increasing throughout Latin America and the Caribbean.
- At least 10% of annual maternal deaths in Latin America and the Caribbean are due to unsafe abortion.
- An estimated 760,000 women in Latin America and the Caribbean are treated annually for complications during or following an unsafe abortion.10
The majority of Latin American countries have very specific restrictions for legal abortion. Mexico is the single largest country of origin for female immigrants in the United States.11 In Mexico, legality of abortion varies by state or county and thus some people believe that it works the same way in the U.S.
As shown in the table on the right, countries and territories in Latin America and the Caribbean can be classified into six categories, according to the circumstances under which abortion is legal.
| Circumstance for Legal Abortion | Coutries with this Circumstance |
|---|---|
| Prohibited altogether, or no explicit legal exception to save the life of a woman | Chile, Dominican Republic, El Salvador, Honduras, Nicaragua |
| To save the life of a woman | Brazil (a), Guatemala, Mexico (a, d, g), Panama (a, d, f), Paraguay, Venezuela |
| To preserve physical health (and save a woman’s life*) | Argentina (a), Bolivia (a, c), Costa Rica, Ecuador (b), Perú |
| To preserve mental health (and all of the above reason) | Colombia (a, c, d) |
| Socioeconomic reasons (and all of the above reasons) | Belize (d) |
| Without restriction as to reason | Cuba (f), Puerto Rico, Uruguay |
U.S. Latinx Communities and Abortion
Latinxs in the U.S. face significant barriers to abortion services. Latinas, in particular, have the lowest rate of health insurance coverage of women of any other racial or ethnic group. For decades, Latinxs have been the most uninsured racial and ethnic group. Because of the Affordable Care Act (ACA), over 4 million Latinx individuals have gained health insurance, lowering the uninsurance rate of the Latinx community from over 40 percent to about 31 percent.13 Latinxs face added barriers to reproductive healthcare, including lack of affordable insurance options, poverty, lack of culturally and linguistically appropriate care, fear of apprehension by immigration enforcement, and bans on abortion access for women being held in immigration detention. Latinxs are more likely to work in low-wage sectors of the economy, including service and agriculture, and for small firms, which are less likely to offer health coverage to their employees.
While not all Latinxs are immigrants, a large portion of immigrants to the U.S. are from Latinx countries, and understanding the intersection of immigration and reproductive health is important context.
- Immigrant women make up 13% of the total female population in the U.S.,14 yet experience some of the most persistent barriers to comprehensive reproductive healthcare services, such as access to contraception or consistent visits to providers.15
- Women composed 46 percent of the 11.4 million unauthorized immigrants in the United States in the 2008-12 period.16
- In the U.S., roughly 45% of immigrant Latin@s and 55% of non-citizen Latin@s do not have healthcare insurance,17 even after implementation of the ACA.
- Federal policies make it nearly impossible to access abortion care in immigration detention, despite the fact that many detainees are women of reproductive age and that 60–80% of Central American women experience sexual assault crossing the U.S.-Mexico border18 and inside detention facilities themselves.
Because immigrants are as diverse a group as any, reporters should steer clear of writing about immigrant communities as if they are from one region, religion, or cultural background, and instead note the wide range of immigration “statuses” and consequently the disparate healthcare options afforded different populations. When reporting on various Latinx communities, it is important to consider the legality and attitudes about abortion in their country of origin, and to remain open to how legality and culture may affect personal beliefs or engagement with reproductive healthcare services here. (See the sidebar, “Medication Abortion (the abortion pill).”)
Medication Abortion (the Abortion Pill)
Medication abortion or abortion with pills can be a safe and effective method when taken according to evidence-based recommendations. Other people live in parts of the country where the medication is not available and there are no abortion providers nearby. In these cases, some women get the mediation themselves through other means and have then used the medication effectively on their own.19
Reproductive health service providers, community-based organizations, and women’s health and rights advocates in the U.S. have reported on the the use of misoprostol in order to self-administer abortion outside of the clinic setting.20 In Latin America, women have been using misoprostol for safe self-administered abortions for over two decades.21,22 As misoprostol became more widely used across Latin America, the use of highly unsafe and invasive abortion methods gradually became less frequent.23,24
While clinic-based abortions will always be an essential component of abortion care, some pregnant people seek medication abortions outside of the formal healthcare system.25
Distance, cost, language barriers, abortion restrictions, and immigration checkpoints are just some of the obstacles that may keep Latinxs from accessing an abortion clinic. We need to expand access to a broader range of abortion options in order for our communities to regain control over their health and lives.26
When a person has decided to have an abortion, they should be able to end their pregnancy in a timely, safe, and affordable manner. Yet, anti-abortion politicians across the United States have quietly passed laws that push abortion out of reach, by restricting the use of medication abortion and enacting requirements that force clinics that provide abortion care to close. This means people in many places in the U.S. have almost no options for abortion care from a trained medical provider. As history has shown, when abortion is stigmatized, made unaffordable, or put out of reach by politicians, there are people who will seek to end their pregnancies on their own. Over the past two years, several women have been charged with murder and sentenced to prison after trying to end their own pregnancies and then seeking medical help. This goes too far. No one should fear arrest or jail for ending their own pregnancy or for seeking medical help in this situation.27
Reporting on Abortion and the Law

Legal Rights, But Limited Access
In the 1973 Roe v. Wade decision, the U.S. Supreme Court found that women, in consultation with their physicians, have a constitutionally protected right to abortion in the earlier stages of pregnancy—that is, before viability, which is estimated at around 24 weeks gestation28—free from government interference. Despite this groundbreaking decision, many women in the United States have never had true access. State-level policies like mandatory waiting periods, exclusion of abortion coverage in Medicaid and other health insurance plans, parental involvement laws, targeted regulation of abortion providers (known as TRAP laws), and similar barriers disproportionately affect young women, low-income women, and people living in rural communities by limiting their ability to find and afford safe and legal abortion.
Since the passage of the Hyde Amendment in 1976, Congress has implemented bans that deny abortion coverage, effectively withholding abortion access from people who qualify for Medicaid and Medicare, military families, federal employees and their dependents, Peace Corps volunteers, Native Americans, women in federal prisons and immigration detention centers, and residents of the District of Columbia.
Incomplete: Roe v. Wade guaranteed women the right to an abortion.
More Accurate: Despite the landmark decision in Roe v. Wade, which granted the right to legal abortion, many barriers, exist especially for those living in poverty, living in rural areas, or living in states that have used multiple strategies to restrict access to the procedure.
The Hyde Amendment and Other Funding Bans
Congress first passed the Hyde Amendment in 1976 (just three years after Roe v. Wade), and the amendment renews annually in the federal appropriations process. The Hyde Amendment prohibits federal funding for Medicaid coverage of abortion care, except when a person is pregnant as a result of rape or incest or when the pregnancy endangers the person’s life. Though Medicaid covers a range of pre- and post-natal care, Congress prohibits Medicaid from covering abortion in nearly all circumstances, and abortion is the only medical procedure banned from the Medicaid program in this way. States can opt to supplement Medicaid funding with state funds in order to provide abortion coverage for Medicaid enrollees, though few have done so. Congress’s yearly reauthorizations of the Hyde Amendment have varied in permitting abortion for life-threatening pregnancies or those caused by rape or incest.
Denial of abortion coverage has a profoundly harmful effect on people and families, particularly those already struggling to make ends meet. (See sidebar, “Rosie Jiménez: The First Victim of Hyde.”) For those who qualify and enroll in Medicaid, the cost of ending a pregnancy forces many people to make impossible decisions—decisions such as keeping food on a family table or paying for needed healthcare. For others, cost is an ultimately insurmountable barrier.
- Over 9 million women of reproductive age—nearly 1 in 7—are insured by Medicaid.30
- A woman who attempts to access abortion services but is denied, is three times more likely to fall into poverty than a woman who is able to get the care she needs.31
- Of low-income women on Medicaid who seek abortion care, 1 in 4 are unable to afford the out-of-pocket costs and are forced to carry the pregnancy to term.32
It is also noteworthy that Latinxs support repealing Hyde. According to polling data released in September 201633:
- Of Latin@ voters in battleground states, 60% support a bill that would require Medicaid to cover all pregnancy-related care, including abortions.
- Of Latin@ voters in battleground states, 75% agree with the statement, “however we feel about abortion, politicians should not be allowed to deny a woman’s health coverage for it just because she’s poor.”
Rosie Jiménez: The First Victim of Hyde
Immigrant women face specific barriers in accessing Medicaid. Immigrants authorized to work and live in the United States face a 5-year waiting period before they can qualify for and receive Medicaid—even if they would qualify solely based on their income.29 In 2012, 19.1 percent of immigrants lived in poverty, the largest group being the 3.2 million people who emigrated from Mexico. These factors mean that millions of Latinx families are among the least likely to be able to afford out-of-pocket healthcare, whether for abortion services or any other type of care, and more likely to qualify for public insurance programs. Hyde doubly impacts immigrant Latinxs by putting abortion access out of reach even after the end of the 5-year coverage restriction.
Rosie Jiménez, a young, working class, Chicana student and single mother, was the first victim of the Hyde Amendment in 1977. She was six months away from graduating with her teaching credential when she found out she was pregnant. Rosie visited a doctor in her hometown of McAllen, TX, seeking an abortion. He refused to perform the procedure because Medicaid no longer reimbursed for abortion care. Desperate and with little cash, Rosie went to Mexico where she obtained an unsafe, illegal abortion. She died from the illegal procedure soon after.
Latinxs’ Views on Abortion
Reporting on racial inequities in who obtains abortion services without exploring the larger context often leads to inaccurate stories that perpetuate myths and stereotypes about communities of color, especially Latinxs.
In the United States, women of color are regularly targeted for scrutiny and policing of their reproductive health decisions by both policymakers and through popular culture. Examples include a billboard campaign targeting Latinas and Black women to convince them to support the efforts to make abortion illegal.
Abortion is illegal or severely restricted in the majority of Latin American countries, and country of origin may influence various communities’ beliefs about abortion once in the United States. Considering how beliefs and experiences of reproductive healthcare from the country of origin still impact women’s decisions and attitudes is an important factor in understanding data about reproductive health.
Even with this context, the data show high support for abortion access across Latinx communities.34
- Of Latin@ voters, 82% believe women should make their own decisions when it comes to abortion.
- Despite some church leaders’ anti-abortion views, 60% of Latin@s agree that abortions should remain legal.
- Of Latin@ voters, 89% say they would offer support to a loved one who had an abortion.
- Of Latin@ voters, 50% agree with the statement, “my personal religious values can support a woman making her own decision about abortion.”
Some recent polls about abortion access and public opinion include:
Latinx Youth Access to Abortion
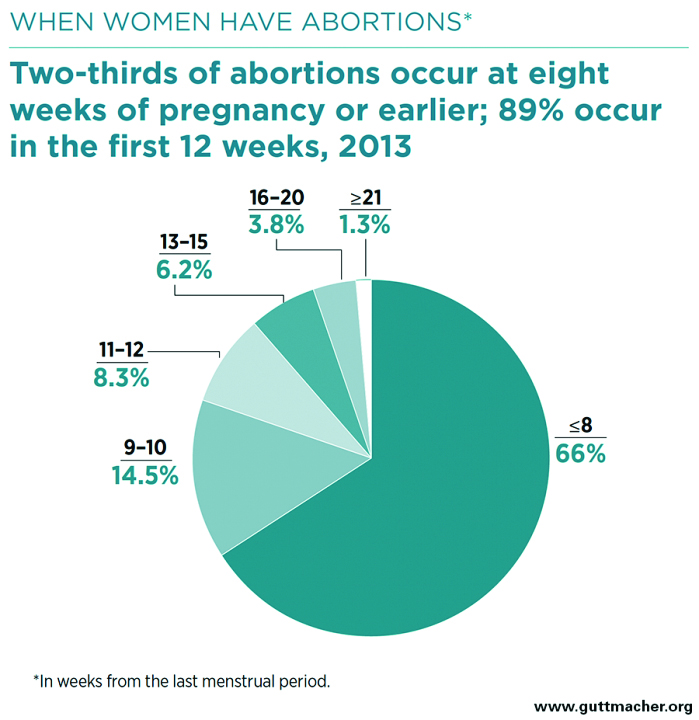
Public discussions of abortion often focus on adolescents, creating the impression that most abortion patients are teenagers, yet the vast majority of women having abortions are 20 years old and older.35 Trends in reporting about teen pregnancy often reinforce these false but popular stereotypes. In reality, recent data show:
- The pregnancy rate among young Hispanic women has steadily declined since the 1990s.36 In 2011, the abortion rate for young Hispanic women was 12.7 per 1,000 women aged 15 to 19.
- Even though stereotypes about teen pregnancy must be dispelled, young people have very real reproductive health needs.
- Even with increased birth control use, nearly 82% of all pregnancies among young people are unintended.37
From a policy-making perspective, adolescents and minors face the harshest restrictions in accessing abortion services. As of August 2016, laws in 38 states require a minor seeking an abortion to involve one or both parents in the decision.38 Most young women do consult their parents before seeking abortion care, but those who do not may face dangerous circumstances at home. Fifty percent of pregnant teens have experienced violence; 30 percent of teens who do not tell their parents about their abortions feared violence or being forced to leave home.39
Given that the procedure is relatively rare for young people, reporters should delve into the challenges young people may face that hinder access to safe and confidential abortion care. To provide a more accurate picture, reporting on young people’s access to abortion should take into consideration the rarity of a person under 20 seeking the procedure, while highlighting the circumstances under which they do. A popular criticism is that ensuring youth access to abortion is promoting abortion. Instead, the goal of reproductive justice advocates is to ensure every person has affordable access to the information and services they need to make reproductive health decisions. That includes comprehensive sex education, as well as contraception, prenatal, maternity, and abortion care. Reporting about abortion and youth sexuality must consider the variety of social factors affecting young Latinx people. A well-rounded discussion does not rely on blame and judgment, and instead examines the conditions young people face that impact their health and safety. (See the sidebar, “Youth, Abortion, and Stigma.”)
Youth, Abortion, and Stigma
While we highlight the declining rates of abortion for young people, it is important that coverage doesn’t judge or stigmatize pregnant and parenting youth. Additionally, it is important not to shame teen sexuality.
“The dominant perspective on youth sexuality has failed to consider the broad context of young Latinas’/os’ lives as it centers on changing individual behavior and erroneously leaves out the role of their social, economic and political environments. Placing the blame for adolescent pregnancy solely on the behaviors/decisions/choices of youth is not only unjust, it fails to tackle the systemic health, educational and economic inequities that may lead to such outcomes. This focus also paints a hetero-normative picture of Latina/o youth sexuality that excludes lesbian, gay, transgender and queer youth altogether. It is time to discuss Latina/o youth sexuality in the context of the many factors in their lives with the goal of strengthening families and communities.”40
—California Latinas for Reproductive Justice report, “Justice for Young Families”
Shame, Stigma, and Reproductive Health
While abortion is one of the safest and most common gynecological procedures that women experience, societal beliefs about the “proper” role of women and women’s sexual behaviors may result in shame and stigma. Individuals who have had an abortion can worry about judgment from others, isolation, self-judgment, and community condemnation.41 The way media frames an issue can greatly influence public opinion and discourse. When politicians use social issues like abortion to incite divisive rhetoric, it is critical that media provide context and facts. Instead, coverage of abortion often perpetuates stigma and misinformation.
Reporters should avoid attempting to describe the “types” of individuals who have abortions or speculating about the cultural reasons why some groups obtain them more than others. Rather, reporting can include background on the many factors and circumstances that contribute to an individual’s decision about an unintended pregnancy as well as relevant data on income and healthcare access, while avoiding stereotypical traps by referencing sexual behavior or decision making.
Storytelling is one way abortion advocates have been shifting a culture of shame towards one of compassion and support for basic healthcare rights. Considering that nearly a third of women in the United States will have an abortion by age 45, abortion storytelling takes this common experience out of isolation and asserts the humanity of the women having abortions. One comprehensive survey of 16 major print and online media outlets showed that abortion is regularly covered as a political issue more than as a health issue, and that women experiencing abortion are rarely present in the coverage.42 The survey also found that in all stories covering abortion between 2014 and 2015 there were no personal stories of Latinas, or any women of color.43 Campaigns like Advocates for Youth’s “1 in 3,” “The Abortion Diary” podcast, or “Shout Your Abortion” provide outlets for people to share their abortion stories and be in community with others who may feel silenced or afraid.
Shame and stigma also affect access to reproductive healthcare, including abortion. Many people—not only women, but also transgender men, intersex, and gender-nonconforming people, and others—can get pregnant and need access to a full range of reproductive health options, including abortion. However, 42 percent of transgender men have experienced verbal harassment, physical assault, or denial of equal treatment in a doctor’s office or hospital.44 Many transgender individuals report that they must teach their medical providers about transgender care.45 In reproductive healthcare and abortion care, transgender men are often an invisible population. Barriers to care include lack of culturally competent service providers, assumptions and stereotypes about gender identity and sexuality, and lack of legal protections to protect trans patients from discrimination.
Journalists must be vigilant in verifying data that supports abortion claims. Groups trying to restrict abortion often cite discredited or misrepresented research on its impact on women. Exhaustive reviews by panels convened by the U.S. and British governments have concluded, for example, that there is no association between abortion and breast cancer. There is also no indication that abortion is a risk factor for other cancers.46 Claims of depression or other emotional distress caused by an abortion have also been widely disputed by medical authorities, who find these effects can be attributed primarily to the impact of shame and stigma on those who have had an abortion, rather than to the procedure itself. In an effort to provide a balanced perspective, journalists should exercise caution that they do not take medically inaccurate claims at face value and ensure they are not comparing them to medically sound arguments.
Other reproductive issues can bring on similar feelings of shame and stigma, such as being a young parent, having a sexually transmitted infection (STI), or expressions of sexuality and gender identity. Reporters covering reproductive justice issues like these have an opportunity to share wider context of individual lives and important health data that help build readers’ understanding and curb unnecessary judgment while reporting the facts.
Incomplete: She had a sexually transmitted infection.
More accurate: Similar to more than one in six people between the ages 14 and 45 in the U.S., she was diagnosed with genital herpes.
Anti-Choice Organizing
A network of national- and state-level organizations work to undermine access to abortion. These groups include: the American Legislative Exchange Council (ALEC), Americans United for Life, Family Research Council, National Right to Life, National Pro-Life Alliance, and the Susan B. Anthony List, which supports candidates who are opposed to abortion.
These groups have launched an unprecedented attack on abortion access and affordability, and more than 338 abortion restrictions have been enacted since 2010. The 338 state abortion restrictions adopted since 2010—the year anti-abortion forces took control of many state legislatures and governors’ mansions—account for 30 percent of the 1,142 abortion restrictions enacted by states since the 1973 Supreme Court decision in Roe v. Wade.47 We anticipate an even greater increase in restrictive federal legislation under the Trump administration which has attacked abortion and healthcare access since day one.
In addition to policy-oriented groups, radical anti-choice groups like Operation Rescue, Live Action, and the Center for Medical Progress engage in deceptive and misleading campaigns using undercover video, surveillance, and sting operations to undermine abortion providers and to stimulate outrage amongst conservative legislators to further restrict access to abortion.
The increasingly hostile policy climate and in-your-face actions of radical anti-choice groups create a climate where threatening and targeting abortion providers and abortion clinic staff can thrive. In a recent study of national clinic violence,48 over 50 percent of clinics report threatening and intimidating behaviors, including “wanted” style posters, leaflets featuring doctors’ photographs and home addresses, and aggressive blockades.
There continues to be a need for the media to distinguish between opposing viewpoints on issues like abortion, and the incendiary rhetoric and misinformation that critics of reproductive health services use. While inflammatory quotes might be newsworthy, their use should be avoided in a story that strives to be objective. This is increasingly important as we enter a time when there is a strong government effort to reduce and eliminate abortion access, and media has a significant role in disputing fake news.
When covering a debate about abortion policies, reporters often refer to those who advocate for access to abortion as pro-choice while those who would eliminate the right as pro-life. These labels skew the perspectives of both individuals and organizations quoted in news coverage, offering a stereotype rather than an accurate portrayal.
Incomplete: abortion advocates, pro-abortion, pro-life
More accurate: reproductive health advocates, those seeking to restrict abortion
Appendix
Terminology
abortion: Abortion includes any medical procedure used to terminate pregnancy. There are different methods of abortion commonly performed depending on length of pregnancy. One is through a medication and the other methods are procedures that take place in a clinic, including aspiration (the most common method) and dilation and evacuation (D&E).49
abortion after 12 weeks: Abortions beyond a specific point (such as 20 weeks postfertilization or the third trimester) have been called “later abortion” or “later-term abortion.”50 These phrases similar to “partial birth abortion” are evocative, highly politically charged terms that have no actual medical definition. While abortion is constitutionally permissible up to the time of viability, state and federal legislators continue to introduce bills to ban abortion after 6, 12, or 20 weeks.51 Communications on these types of bans should avoid eliciting a visceral response, and move away from the phrases “later” or “late-term” or “partial-birth” abortions. When appropriate use: “as a pregnancy progresses,” “at different points in pregnancy,” and “after 12 weeks” to describe abortion later in a pregnancy.
fetus: A fetus is defined from 8 weeks after conception until term while in the uterus.52
medication abortion: An abortion using the medication mifepristone, which is prescribed by a medical provider, is a medication abortion. A woman can take this medication in the first 10 weeks of pregnancy.53
surgical abortion: There are several forms of surgical abortion. The most common type of surgical abortion in the U.S. is done by aspiration. It is performed in a clinic or hospital, and can be used up to 16 weeks after the person’s last period.54
unintended pregnancy: A pregnancy may be mistimed, unplanned, or unwanted at the time of conception.55
viability: Roe v. Wade developed a trimester framework for gestational age, and declared that abortions in the third trimester could only be performed if the health of the mother was in jeopardy, implying that a fetus was legally viable at 28 weeks. Since Roe was passed, the legal definition of viability has been delegated to individual states. States often rely on the attending physician to determine viability. For states that define viability, the limit ranges from 19 to 28 weeks.56
Endnotes
- Reichard, R. (2015). Why we say Latinx: Trans and gender non-conforming people explain. Retrieved from: http://www.latina.com/lifestyle/our-issues/why-we-say-latinx-trans-gender-non-conforming-people-explain
- Ross, L.(n. d.). Bring human rights home. Makers. Retrieved from: http://www.makers.com/moments/new-paradigm-reproductive-justice
- Roberts, D. (2015). Reproductive justice, not just rights. Dissent. Retrieved from: https://www.dissentmagazine.org/article/reproductive-justice-not-just-rights
- Forward Together (formerly Asian Communities for Reproductive Justice). (2005). A new vision for advancing our movement for reproductive health, reproductive rights and reproductive justice. Retrieved from: http://forwardtogether.org/assets/docs/ACRJ-A-New-Vision.pdf
- Ibid.
- Ibid.
- Ross, L. (2006). What is reproductive justice? Sistersong Reproductive Justice Collective. Retrieved from: https://www.trustblackwomen.org/our-work/what-is-reproductive-justice/9-what-is-reproductive-justice
- Guttmacher Institute. (2017). Fact sheet: Induced abortion in the United States. Retrieved from: https://www.guttmacher.org/fact-sheet/induced-abortion-united-states
- Guttmacher Institute. (2016). Abortion in Latin America and the Caribbean: Incidence and trends. Retrieved from: https://www.guttmacher.org/fact-sheet/facts-abortion-latin-america-and-caribbean
- Ibid.
- American Immigration Council. (2014). Fact sheet: Immigrant women in the United States, a portrait of demographic diversity. Retrieved from: https://www.americanimmigrationcouncil.org/research/immigrant-women-united-states-portrait-demographic-diversity
- Center for Reproductive Rights (CRR). (2016). The world’s abortion laws. Retrieved from: http://worldabortionlaws.com/
- Obama, B. (2016). Presidential proclamation—National Hispanic Heritage Month, 2016. Retrieved from: https://obamawhitehouse.archives.gov/the-press-office/2016/09/15/presidential-proclamation-national-hispanic-heritage-month-2016
- American Immigration Council. (2014). Fact sheet: Immigrant women in the United States, a portrait of demographic diversity. Retrieved from: https://www.americanimmigrationcouncil.org/research/immigrant-women-united-states-portrait-demographic-diversity
- Strong Families. (2015). Immigrant communities and abortion. Retrieved from: http://strongfamiliesmovement.org/rj-immigrant-access
- Migration Policy Institute. (2015). Immigrant women in the United States. Retrieved from: http://www.migrationpolicy.org/article/immigrant-women-united-states#Unauthorized%20Population
- National Latina Institute for Reproductive Health. (2015). Immigrant Latin@s & abortion: The fight for access to comprehensive coverage and care, fact sheet. Retrieved from: http://latinainstitute.org/sites/default/files/NLIRH_ImmWmnAbrtn_FactSheet_Eng_R6.pdf
- Siegal, E. M., & Bonello, D. (2014). Is rape the price to pay for migrant women chasing the American Dream? Fusion. Retrieved from: http://fusion.net/story/17321/is-rape-the-price-to-pay-for-migrant-women-chasing-the-american-dream/
- COMS Project. (2016). Wayfinder: Self-induced abortion. For access, email: hello@COMSProject.org
- Grossman, D., Holt, K., Pena, M., Lara, D., Veatch, M., Cordova, D., Gold, M., Winikoff, B., & Blanchard, K. (2010). Self-induction of abortion among women in the United States. Reproductive Health Matters, 18(36), 136–146. Retrieved from: http://dx.doi.org/10.1016/S0968-8080(10)36534-7
- Lafaurie, M. M., Grossman, D., Troncoso, E., Billings, D. L., & Chávez, S. (2005). Women’s perspectives on medical abortion in Mexico, Colombia, Ecuador, and Peru: A qualitative study. Reproductive Health Matters, 13(26), 75–83. DOI: 10.1016/S0968-8080(05)26199-2 Retrieved from: http://dx.doi.org/10.1016/S0968-8080(05)26199-2
- Barbosa, R., & Arilha, M. (1993). The Brazilian experience with Cytotec. Studies in Family Planning, 24(4), 236–240. Retrieved from: https://www.jstor.org/stable/2939191?seq=1#page_scan_tab_contents
- Lafaurie, M. M., Grossman, D., Troncoso, E., Billings, D. L., & Chávez, S. (2005). Women’s perspectives on medical abortion in Mexico, Colombia, Ecuador, and Peru: A qualitative study. Reproductive Health Matters, 13:(26), 75–83. DOI: 10.1016/S0968-8080(05)26199-2 Retrieved from: http://dx.doi.org/10.1016/S0968-8080(05)26199-2
- Barbosa, R., & Arilha, M. (1993). The Brazilian experience with Cytotec. Studies in Family Planning. 24(4), 236–240. Retrieved from: https://www.jstor.org/stable/2939191?seq=1#page_scan_tab_contents
- Adams, J. E., & Mikesell, M. (n.d.). Primer on self-induced abortion, the SIA Legal Team. Retrieved from: https://www.law.berkeley.edu/wp-content/uploads/2016/01/SIA-Legal-Team-Primer.pdf
- Ibid.
- COMS Project. (2016). Wayfinder: Self-induced abortion. For access, email: hello@COMSProject.org
- The American Congress of Obstetricians and Gynecologists. (2012). ACOG statement on HR 3803. Retrieved from: http://www.acog.org/~/media/Departments/Government%20Relations%20and%20Outreach/20120618DCAborStmnt.pdf
- Healthcare.gov. (n. d.). Coverage for lawfully present immigrants. Retrieved from: https://www.healthcare.gov/immigrants/lawfully-present-immigrants/
- Ibis Reproductive Health. (n. d.). Research brief: The impact of Medicaid coverage restrictions on abortion. Retrieved from: http://allaboveall.org/wp/wp-content/uploads/2014/08/MedicaidResearchBrief.pdf
- Strong Families. (2015). Reproductive Justice Media Guide, The Hyde Amendment and other funding restrictions, Retrieved from: http://strongfamiliesmovement.org/rj-hyde
- Bridges, E. (2014). Abortion and young people in the United States. Advocates for Youth, January 2014 http://www.advocatesforyouth.org/publications/publications-a-z/2296-abortion-and-young-people-in-the-united-states
- Heart Research Associates. (2016). Battleground pollling on repealing the Hyde Amendment. Retrieved from: http://allaboveall.org/wp/wp-content/uploads/2016/09/AllAboveAll_Hart_Battleground-Poll-2016-Memo.pdf
- PerryUndem Research/Communication. (2016). Latino/a voters’ views on abortion: Retrieved from: http://latinainstitute.org/sites/default/files/NLIRH%20Public%20Survey%20Report_Final.pdf
- Guttmacher Institute. (2017). Fact sheet: Induced abortion in the United States. Retrieved from: https://www.guttmacher.org/fact-sheet/induced-abortion-united-states
- Guttmacher Institute. (2011). Tables. Retrieved from: https://www.guttmacher.org/sites/default/files/report_downloads/us-teen-pregnancy-trends-2011_tables.pdf
- Mosher, W.D., & Jones, J. (2010). Use of contraception in the United States: 1982–2008. National Center for Health Statistics. Vital and Health Statistics, 23(29). Retrieved from: https://www.cdc.gov/nchs/data/series/sr_23/sr23_029.pdf
- Guttmacher Institute. (2016). American teens’ sexual and reproductive health. Retrieved from: https://www.guttmacher.org/fact-sheet/american-teens-sexual-and-reproductive-health
- Bridges, E. (2014). Abortion and young people in the United States. Advocates for Youth. Retrieved from: http://www.advocatesforyouth.org/publications/publications-a-z/2296-abortion-and-young-people-in-the-united-states
- Valladares, E. S., Valle, G., & Jiménez, L. (Eds.). (2012). Supporting Latina/o youth: Strengthening Latina/o young families and communities. California Latinas for Reproductive Justice. Retrieved from: http://www.californialatinas.org/wp-content/uploads/2012/08/CLRJ_Supporting_Latina_O_Youth_Issue_Brief_1_FINAL.pdf
- Cockrill, K., Upadhyay, U. D., Turan, J., & Foster, D. G. (2014). The stigma of having an abortion: Development of a scale and characteristics of women experiencing abortion stigma. Perspectives on Reproductive and Sexual Health, 45(2), 79–88. Retrieved from: https://www.guttmacher.org/journals/psrh/2013/05/stigma-having-abortion-development-scale-and-characteristics-women
- Nixon, L., Seklir, L., Mejia, P., Cockrill, K., Herold, S., Woodruff, K., & Dorfman, L. (2017). Shaping stigma: An analysis of mainstream print and online news coverage of abortion, 2014–2015. Issue, 23, 1–36. Berkeley Media Studies Group. Retrieved from: http://seachangeprogram.org/wp-content/uploads/2017/01/bmsg_sea_change_issue23_abortion_stigma2017.pdf
- Ibid.
- Seaman, A. M., (2015). Transgender people face discrimination in healthcare. Reuters Health. Retrieved from: http://www.reuters.com/article/us-transgender-healthcare-discrimination-idUSKBN0M928B20150313
- Grant, J. M., Mottet, L. A., &, Tanis, J. (Leads). (with Harrison, J., Herman, J. L., & Keisling, M.) (2011). Injustice at every turn: A report of the National Transgender Discrimination Survey. The National Gay and Lesbian Task Force and the National Center for Transgender Equality. Retrieved from: https://calculators.io/national-transgender-discrimination-survey/
- Guttmacher Institute. (2017). Fact sheet: Induced abortion in the United States. Retrieved from: https://www.guttmacher.org/fact-sheet/induced-abortion-united-states
- Guttmacher Institute. (2017). Policy Trends in the States: 2016. Retrieved from: https://www.guttmacher.org/article/2017/01/policy-trends-states-2016
- Feminist Majority Foundation. (2014). National clinic violence survey. Retrieved from: http://feminist.org/rrights/pdf/2015NCAPsurvey.pdf
- 1 in 3. (n. d.). Abortion information and resources. Retrieved from: http://www.1in3campaign.org/resources/abortion-information-resources
- Guttmacher Institute. (2017). Evidence You Can Use: Later Abortion. Retrieved from: https://www.guttmacher.org/evidence-you-can-use/later-abortion
- National Latina Institute for Reproductive Health. (2015). Bans on later abortion: A threat to health and dignity, fact sheet. Retrieved from: http://latinainstitute.org/sites/default/files/NLIRH_20WeekBan_FactSheet_Eng_R11.pdf
- Barfield, W. D., & the Committee on Fetus and Newborn. (2011). Clinical reports: Standard terminology for fetal, infant, and perinatal deaths. Pediatrics, 128, 177-181. Retrieved from: http://pediatrics.aappublications.org/content/128/1/177
- Guttmacher Institute. (2017). Fact sheet: Induced abortion in the United States. Retrieved from: https://www.guttmacher.org/fact-sheet/induced-abortion-united-states
- 1 in 3. (n. d.). campaign: Abortion information and resources. Retrieved from: http://www.1in3campaign.org/resources/abortion-information-resources
- Centers for Disease Control and Prevention. (2015). Unintended pregnancy prevention, Retrieved from: https://www.cdc.gov/reproductivehealth/unintendedpregnancy/
- Arzuaga, B., & Lee, B. H. (2011). Pediatrics perspective: Limits of human viability in the US: A medicolegal review. Pediatrics, 128(6), 10471052. Retrieved from: http://pediatrics.aappublications.org/content/128/6/1047.short
Who Made This Guide?
![]()
![]()

![]()

Media inquiries: Janna Zinzi, janna@forwardtogether.org